Breathing new life into lung cancer research
 Brendon Stiles, M.D.
Thoracic surgeon Brendon Stiles, M.D., may be one step closer to a cure for advanced lung cancer than ever before – thanks, in part, to his patients.
Brendon Stiles, M.D.
Thoracic surgeon Brendon Stiles, M.D., may be one step closer to a cure for advanced lung cancer than ever before – thanks, in part, to his patients.
Those undergoing surgery in his operating room at NewYork-Presbyterian/Weill Cornell Medical Center are often active participants in Stiles’s research into the basic biology and mechanisms of lung cancer. While excising their tumors, Stiles biobanks blood and tissues from their diseased lungs as well as their healthy lungs, so that each patient can also serve as their own control in his studies.
The direction for his laboratory investigations often comes directly from discoveries he makes from specimens removed in the operating room. During the analysis of some of his patients’ samples in search of potential biomarkers for lung cancer, for example, Stiles came across one protein in particular that seemed to be expressed and secreted from the surface of many of the cancerous cells: the protein ADP-ribosyltransferase 1 (ART1).
“We found it in the blood while doing proteomics screenings and wondered why it was there,” Stiles said. “We looked back through biobank materials and found it was also prevalent in tumor samples, more so than in matched normal tissue. So we began to investigate whether ART1 has a functional role in lung cancer.”
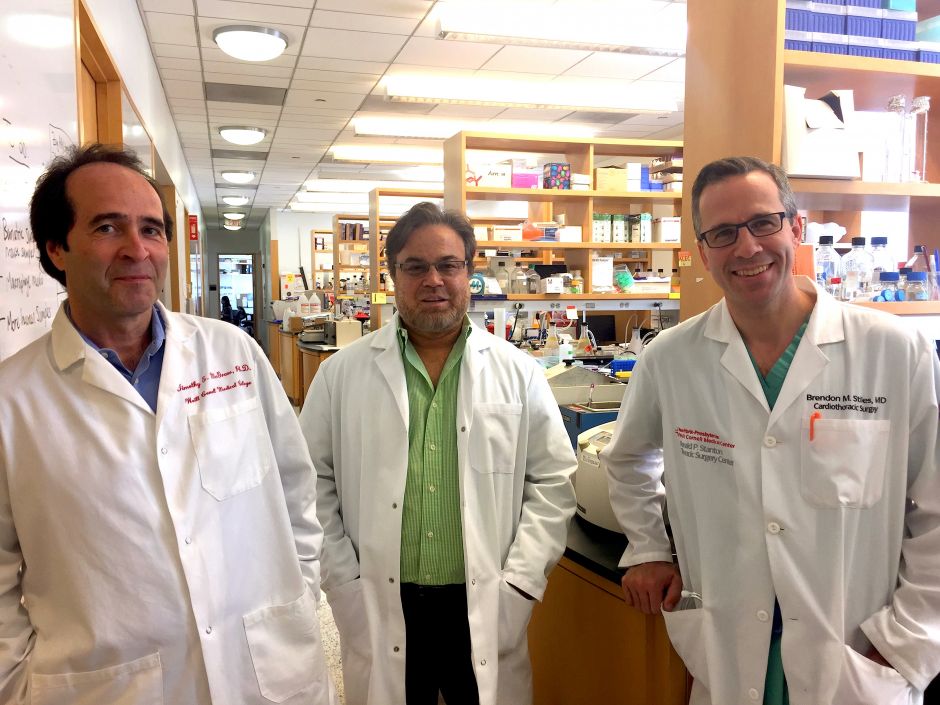
Working with researchers Timothy McGraw, Ph.D., Vivek Mittal, Ph.D., Nasser Altorki, M.D. and other colleagues at the Sandra and Edward Meyer Cancer Center, Stiles knocked down ART1 in cell lines developed from a genetically altered mouse model.
“We saw amazing effects. If you get rid of the protein, the cells struggle to grow tumors and to metastasize in immune competent mice,” Stiles said.
Although not previously described in relation to lung cancer, ART1 has recently been investigated in colon cancer. Targets of extracellular mono-ADP-ribosylation have not been well characterized, but ART1 may affect many biological processes. Stiles said it may interfere with pathways by which neutrophils and lymphocytes try to attack cancer cells, for instance. Suppressing it could help augment the immune response, and boost the effectiveness of immune checkpoint inhibitors such as the anti-PD1 drugs nivolumab and pembrolizumab, which have shown particular promise as treatments for melanoma and non-small cell lung cancer.
He is now further exploring the expression of ART1 in his patients, in particular how it is regulated and secreted on the surface of cancer cells, as well as its link to metastasis.
 Timothy McGraw, Ph.D., Vivek Mittal, Ph.D., and Brendon Stiles, M.D.
Stiles’s team will also look at inhibitors of the protein. There are already a handful of drugs on the shelf that they will test, and they will work with Hening Lin, Ph.D., a professor of chemistry at Cornell University in Ithaca, to develop and test additional compounds.
Timothy McGraw, Ph.D., Vivek Mittal, Ph.D., and Brendon Stiles, M.D.
Stiles’s team will also look at inhibitors of the protein. There are already a handful of drugs on the shelf that they will test, and they will work with Hening Lin, Ph.D., a professor of chemistry at Cornell University in Ithaca, to develop and test additional compounds.
“It might be possible to combine it with a PD-1 inhibitor to get more bang for the buck,” Stiles said. “If not a cure, we may be able to achieve a durable response (where the cancer doesn’t progress for an extended time period).”
His efforts will be boosted by a $600,000 grant from Free to Breathe. Stiles, along with McGraw and Mittal, were recently awarded the organization’s inaugural Metastasis Research Grant.
Stiles said incorporating research into his clinical practice can be challenging, but also rewarding.
“To me, this is a cool way to do science—from the patient, to the bench, and back again to the patient,” Stiles said. “It helps in the clinic as well. Everything in the clinical world happens so fast. Applying basic research principles to clinical questions forces you to slow down, to stop and think about how you can best test a hypothesis.”
He also enjoys being a conduit for patient participation in research.
“Patients are often resistant to taking part in clinical trials or biobanking, but when you can explain exactly what you will be doing, it becomes exciting,” Stiles said. “They like to hear we are empathetic to their problems; they like to hear that someone is trying to do something.”
Stiles works closely with lung cancer survivors and advocacy groups to raise money and awareness. He is on the Medical Advisory Board of the Lung Cancer Research Foundation, and is active on Twitter (as @BrendonStilesMD), where he regularly participates in bi-weekly lung cancer social media (#LCSM) tweetchats. In September, he will be hosting a lab visit for patient and advocate participants of the Free to Breathe Lung Cancer Action Summit.
Not necessarily a death sentence
By the time most lung cancer patients show symptoms, 75 percent will have locally advanced or metastatic disease, with survival rates as poor as 9 percent over five years.
It is possible to catch lung cancer at the earliest stages using low-dose computed tomography (LDCT) imaging. At its earliest stage, 10-year survival after curative surgery can reach 88 percent.
But convincing smokers to get tested can be a challenge.
“There’s such a stigma behind lung cancer,” said Bradley Pua, M.D., director of the NewYork-Presbyterian/Weill Cornell Medical Center Lung Cancer Screening Program. “Fear of what we might find is one of the biggest hurdles. But a diagnosis of lung cancer is not a death sentence if you catch it early.”
 Low-dose CT scans can catch lung cancer before symptoms appear
Weill Cornell Medical College spearheaded lung cancer screening efforts back in 1992, when a group of physicians started the Early Lung Cancer Action Program (ELCAP), which has since expanded into an international network. The results of an extensive study they undertook with colleagues from New York University Medical Center, published in 1999, stimulated research efforts on CT screening for lung cancer throughout the world.
Low-dose CT scans can catch lung cancer before symptoms appear
Weill Cornell Medical College spearheaded lung cancer screening efforts back in 1992, when a group of physicians started the Early Lung Cancer Action Program (ELCAP), which has since expanded into an international network. The results of an extensive study they undertook with colleagues from New York University Medical Center, published in 1999, stimulated research efforts on CT screening for lung cancer throughout the world.
The National Lung Screening Trial, a large randomized trial launched in 2002, screened more than 53,000 current or former smokers and found LDCT imaging was more effective than conventional X-rays, leading to 20 percent fewer deaths from lung cancer, or one life saved per 320 high-risk patients screened.
The healthcare profession – and government – has endorsed annual screenings for those at high risk (adults aged 55-80 years who have a 30 pack-year smoking history and currently smoke or have quit within the past 15 years). Private insurer reimbursement was included as part of the Affordable Care Act in 2014, and the Centers for Medicare and Medicaid Services announced it February that it will also cover screenings. If insurance coverage is not available, the cost of the screening is $350.
Pua re-launched the NYP/Weill Lung Cancer Screening Program in 2014. He has created a comprehensive program, where screening is part of a clinical diagnostic process, not simply a standalone test. He works with a multi-disciplinary team of pulmonologists, oncologists, radiologists and thoracic surgeons, as well as a counselor who leads a smoking cessation program.
Whether patients are sent by a doctor or self-referred, they benefit from the comprehensive care that Cornell offers. Pua said.
“We take them through the entire process, even diagnosis and treatment,” Pua said.
The low-dose CT screening can be performed at four sites throughout New York City on the same day as the initial consultation. Radiologists analyze the results using a state-of-the-art computer-aided three-dimensional diagnosis tool which allows them to measure the volume of any nodules discovered (rather than conventional two-dimensional measurements of cross-sectional diameters) and to assess the aggressiveness of a tumor by calculating its doubling time.
Those results are also delivered on the same day. While the vast majority will be negative, those who receive a positive diagnosis can be counseled on next steps. There are multiple avenues to treat patients at NYP/Weill, including same-day procedures that Pua, an interventional radiologist, can do himself. These include thermal ablation, in which one or two small needles are inserted into a tumor to burn or freeze it.
Around 350 people have been screened in the past year and a half, Pua said. Of those, four were diagnosed with early stage lung cancers. All underwent curative treatment within a matter of weeks.
For other patients, the screenings led to findings about their lung and heart health -- the CT scans can also detect emphysema and coronary artery calcifications.
And, importantly, they create a counseling opportunity that results in greater smoking cessation.
“We’ve converted a lot of smokers by showing them the state of their lungs,” Pua said. “That’s certainly an advantage.”
Pua is currently expanding clinical services in Lower Manhattan in an effort to target underserved Latino and Chinese populations, and his next goal is to add a research component to the program. He recently hired a database manager and epidemiologist, and they will begin by studying additional risk factors such as second-hand smoke.